Commit Suicide Then Rise Again on the Third Day
The suicide rate increased 33 percent from 1999 through 2017, from 10.5 to 14 suicides per 100,000 people (NCHS Data Brief No. 330, November 2018). Rates have increased more sharply since 2006. Suicide ranks equally the quaternary leading crusade of death for people ages 35 to 54, and the second for 10- to 34-twelvemonth-olds. Information technology remains the 10th leading crusade of expiry overall.
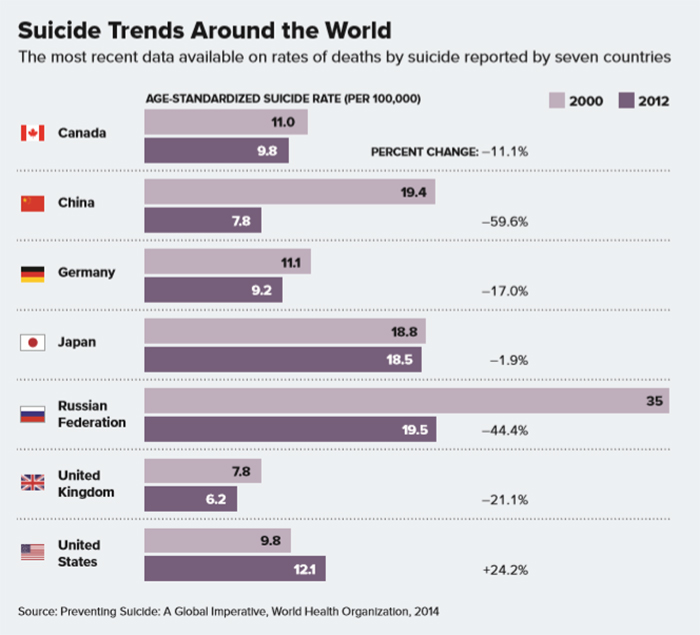
Merely it's a different story in other parts of the earth. Over roughly the same period, other countries have seen rates fall, including Japan, Mainland china, Russian federation and most of Western Europe. What is going wrong on our shores—and what lessons can we import from elsewhere?
Suicide trends: Looking for clues
Pinpointing the reasons that suicide rates ascent or fall is challenging in part because the causes of suicide are complex. Risk factors include health factors (such equally depression, substance use bug, serious mental affliction and serious physical wellness conditions including pain), environmental factors (such as access to lethal means and stressful life events including divorce, unemployment, relationship problems or financial crisis) and historical factors (including previous suicide attempts, a family history of suicide and a history of childhood abuse or trauma).
"At the individual level, at that place is never a single cause of suicide. There are ever multiple risk factors," says Christine Moutier, Doc, chief medical officer of the American Foundation for Suicide Prevention. "That confluence of multiple take chances factors makes information technology a trickier business to explain a population-level rise."
And while the climbing rates are cause for concern, experts indicate out that they don't tell the whole story. In fact, the U.Southward. suicide rate is like today to the rate of xxx years agone. Deaths by suicide fell markedly in the 1980s and 1990s earlier ascension again at the turn of the century. What'south more, while some countries, such as Russia, have seen dramatic declines in suicide rates since the 1990s, their rates are nevertheless well in a higher place those in the United States.
In other words, there is no obvious culprit for an increment in suicides—nor is at that place a single, easy solution we can import from other nations to turn the trend around. Yet there are clues.
Socioeconomic changes might be office of the puzzle. Globally, suicide rates have often fallen when living atmospheric condition accept improved. And the reverse is also true. Princeton University economists Anne Case, PhD, and Angus Deaton, PhD, have shown that deaths from suicide, drugs and booze have risen steeply amidst white, centre-aged Americans since 2000 (PNAS, Vol. 112, No. 49, 2015). They contend these "deaths of despair" are linked to a deterioration of economical and social well-being amid the white working form (Bloodshed and Morbidity in the 21st Century, Brookings Papers on Economical Activity, Spring 2017).
The CDC figures appear in line with that theory. From 2000 to 2016, the suicide rate for white Americans climbed from 11.29 to xv.7. For black Americans, information technology rose from v.52 to vi.03 over the same flow. What's more, suicides have increased most sharply in rural communities, where loss of farming and manufacturing jobs has led to economic declines over the by quarter century.
Meanwhile, people who are struggling often fail to receive interventions that could save their lives. "There is a lack of accessible, affordable, constructive mental health care. And the wellness-care system hasn't been designed with suicide risk in mind," Moutier says.
Limiting legal means
While data from other countries tin't explain the rising rate of American suicides, they may concord clues about how to forestall them. One takeaway from the information both at home and away: Limiting access to means of death can make a real difference.
When countries have made it harder to access a means of death, their suicide rates take declined. In England, people in one case could end their lives with carbon monoxide from toxic coal gas. When the land switched to less-toxic gas for heating and cooking, deaths from suicide dropped by 40 per centum. In Asia, many countries saw suicide rates drop after making it more than hard to access toxic pesticides that are used in farming. Bridge barriers that prevent people from jumping have similar effects.
In the United states, more than one-half of all suicide deaths are the result of firearms. And there's testify that when admission to guns goes down, then do suicide deaths. During the 1990s, household gun ownership fell significantly. During those years, deaths from suicide by firearm also decreased, while suicide past other means stayed most the same. The result: a notable drop in the overall suicide rate, from more 12 per 100,000 in 1990 to simply nether 10.v in 1999.
A strategy for prevention
Another common element among many countries that have seen suicide rates fall: They accept made suicide prevention a mission, through efforts such as improving admission to mental health treatment, investing in community interventions, coordinating suicide prevention across wellness-intendance, social, education and employment services, and implementing workplace suicide prevention programs that railroad train supervisors to identify and help those at hazard. "Some of those countries, including Japan, have gotten impressively serious about investing in a national plan," Moutier says.
Nippon has long had some of the highest suicide rates amidst industrialized countries. Rates there rose markedly in the late 1990s, a tendency oft attributed to the Asian financial crunch of 1997. Effectually the plough of the 21st century, a cultural shift occurred. Japanese citizens began to view suicide every bit a public health problem rather than equally a personal trouble to deal with in private. In 2006, the country passed legislation to fund suicide sensation and prevention campaigns and by 2012, the number of suicide deaths had fallen below 30,000 for the commencement time in more than a decade.
One element of Nihon'due south programme that appears to have been helpful was a mandate requiring that detailed, municipal-level suicide statistics be released every month. That stride immune suicide prevention resources to exist matched to communities with the greatest needs.
In the United States, timely suicide data that include details nearly risk factors and mechanisms of expiry have been hard to come by. The CDC's National Violent Death Reporting Organisation, which collects such details, was only created in 2002, and information technology wasn't until 2022 that it was expanded to collect data on suicides and other violent deaths from all l states. "Nosotros haven't had a really good picture of the characteristics and life experience of suicide decedents beyond the U.S.," says Jane L. Pearson, PhD, chair of the Suicide Research Consortium at the National Establish of Mental Health.
The United States has also been tedious to develop a national strategy. The country'south first national plan to address suicide prevention was published in 2001, and information technology wasn't until 2010 that the National Action Alliance for Suicide Prevention was launched equally a public-private partnership to accelerate and update the National Strategy for Suicide Prevention. That strategy, released by the U.S. Surgeon General and the Action Alliance in 2012, outlines goals and objectives for reducing deaths by suicide.
It'southward an encouraging step, Pearson says, simply in that location's been a lag in moving from research to action to come across the National Strategy objectives. Accessible, affordable mental wellness services are notwithstanding out of reach for many people with suicidal thoughts and behaviors. "We can't indicate to any single gene causing an individual to consider suicide, only we tin point to health-care practices that can make a difference in suicide prevention. The three key areas are take chances identification, intervention and follow-upward," Pearson says. "We're making progress in understanding risk factors and how to intervene, just the rate keeps climbing considering we're not fully implementing what nosotros know."
I promising approach comes from a study past psychologist Edwin Boudreaux, PhD, at the University of Massachusetts Medical School, and colleagues. The multi-site trial explored universal suicide screening in hospital emergency departments. Report participants who were identified as being at adventure received an intervention that involved an cess, brief intervention, discharge resources and follow-upwardly phone calls focused on reducing suicide gamble. Patients who received the screening and intervention had thirty percent fewer total suicide attempts in the next year compared with patients who received treatment as usual (JAMA Psychiatry, Vol. 74, No. half-dozen, 2017).
Such interventions are promising, but there's a lot of work to be done. Meanwhile, Pearson and other experts fence that psychologists should be doing more than to assistance those at take a chance of dying by suicide. Many psychology training programs barely impact the topic, Pearson says. "You'd think mental wellness professionals should be experts in helping suicidal people, but we aren't."
But it's never too late to become up to speed. "There's and then much feet effectually treating suicidal people, merely yous shouldn't beat yourself up. If you trained more than five or x years ago, there wasn't a lot of scientific discipline to inform what we should exist doing clinically," Moutier says. "Now there are new standards to exist aware of." She recommends mental health professionals, physicians and other clinicians familiarize themselves with the standard care recommendations published by the National Action Alliance for Suicide Prevention (Recommended Standard Treat People with Suicide Risk: Making Wellness Care Suicide Safety, 2018).
For professionals working in outpatient behavioral wellness settings, those recommendations include:
- Assessing patients for suicide risk at intake and repeating the assessment periodically.
- Completing a safety program in collaboration with all patients at increased take a chance during the aforementioned visit.
- Giving patients information on telephone crisis lines.
- Taking steps to reduce access to lethal means, including asking family members to assist.
- Reassessing risk and reviewing or updating the safety plan at each visit until the take chances is reduced.
A key message, experts say, is that there is 18-carat promise for people because suicide. "Suicide is near despair, and the just cure for despair is hope," says Joel Dvoskin, PhD, ABPP, a clinical and forensic psychologist in Arizona and New Mexico who has worked with jails to implement suicide prevention interventions amid inmates. "Psychologists tin can prevent suicide by helping people to regain hope. If we're not virtually that, nosotros should get out of the business."
Source: https://www.apa.org/monitor/2019/03/trends-suicide
{kind=link}
Post a Comment for "Commit Suicide Then Rise Again on the Third Day"